Hyponatremia is when the sodium level in the blood is too low. It is one of the most common electrolyte disorders.
What is hyponatremia?
The most common triggers for hyponatremia are excessive drinking of water, water overload from gastric lavage, psychogenic polydipsia, use of certain medications such as diuretics or ACE inhibitors, as well as severe diarrhea and renal salt depletion. See AbbreviationFinder for abbreviations related to Hyponatremia.
Hyponatremia is when the sodium level is too low. This leads to a reduced concentration of sodium ions in the blood. The concentration drops to values below 135 mmol/l. In severe cases, even life-threatening attacks of hyponatremia are possible, which require immediate treatment in a hospital. Hyponatraemia is one of the most common electrolyte disorders.
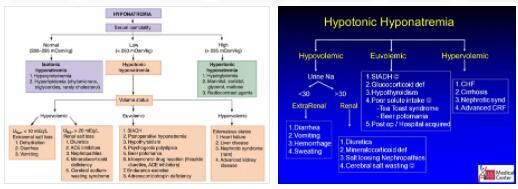
It appears in 15 to 30 percent of all patients who undergo inpatient therapy. The onset of hyponatraemia prolongs the patient’s hospital stay because the clinical prognosis worsens. However, athletes can also be affected by the electrolyte imbalance if they consume an excessive amount of liquid before a competition. There are several forms of hyponatremia: hypovolemic, normovolemic and hypervolemic hyponatremia.
In the case of hypovolemic hyponatraemia, the increase in sodium concentration is accompanied by reduced blood volume. A typical identifying feature is the lower central venous pressure, which is noticeable when the veins in the neck are empty. We speak of normovolemic hyponatremia when the blood volume is normal with the increased sodium concentration.
Hypervolemic hyponatremia is a combination of increased sodium concentration and reduced blood volume. This increases the central venous pressure.
Causes
Hyponatremia is initially assumed to be caused by a sodium deficiency. However, the electrolyte imbalance is triggered by a relative excess of water in the body. During this process, the organism no longer properly excretes pure water through the kidneys. In relation to the sodium concentration in the body, the excess water in the blood turns out to be too high.
The volume of the extracellular fluid is determined by the water of solution of the sodium ions as well as their counterions such as chloride. In the intracellular fluid, on the other hand, potassium is predominant. In the case of a rapidly occurring sodium deficiency, the oncotic pressure drops. The water now flows into body cells, in which there is initially a higher oncotic pressure, which results in an increase in cell volume. This, in turn, can lead to an increase in pressure in the brain. The symptoms of the disease then correspond to the symptoms that occur with increased intracranial pressure. However, if the hyponatremia develops slowly, this does not occur.
The most common triggers for hyponatremia are excessive drinking of water, water overload from gastric lavage, psychogenic polydipsia, use of certain medications such as diuretics or ACE inhibitors, as well as severe diarrhea and renal salt depletion. But diseases such as pituitary insufficiency, hypothyroidism or adrenal insufficiency are also possible causes.
Symptoms, Ailments & Signs
One problem with hyponatremia is its unspecific symptoms, which often lead to misdiagnoses. These include muscle spasms, seizures, lethargy, loss of appetite, confused behavior, and disorientation. Even a coma is a possibility. Cerebral edema occurs with rapidly progressing hyponatremia. This is noticeable through tremors, nausea, headaches and epileptic seizures.
On the other hand, if the electrolyte disturbance occurs slowly, the patient initially suffers from confusion and fatigue for two days. There are also changes in his personality. If hyponatremia takes a chronic form, gait disorders and frequent falls often occur. Since the electrolyte imbalance also has a negative effect on the mineralization of the bones, there is a tendency to bone loss (osteoporosis), which in turn increases the risk of bone fractures.
Diagnosis & course of disease
Hyponatraemia is usually diagnosed by determining the serum sodium value. Other important parameters are urine osmolality, serum osmolality, extracellular volume status and urine sodium concentration. Determining these parameters must be done as quickly as possible.
Exclusion diagnostics also play an important role. So it is important to rule out other diseases that may be causing the symptoms. This could be kidney or thyroid disease. The course of hyponatremia depends on the extent of the electrolyte disturbance. In severe cases, complications such as central pontine myelinolysis, which damages the covering of nerve fibers within the brainstem, can occur.
Complications
Hyponatremia can cause a variety of symptoms. Complications and symptoms usually depend on the actual sodium levels in the blood and for this reason can also vary. The patient usually feels ill and suffers from a loss of appetite. Furthermore, the affected person appears confused and can no longer concentrate and coordinate properly. The muscles ache and it is not uncommon for cramps and nausea to occur.
As the hyponatremia progresses, the patient may experience epileptic seizures and severe headaches. It is not uncommon for gait disorders and fatigue to occur. The person concerned is no longer resilient and feels defeated. The patient’s quality of life is significantly reduced by the hyponatremia.
The treatment of hyponatraemia is always causal and depends on the underlying disease. Usually there are no further complications. The symptoms can be resolved with the help of solutions and infusions. If the person concerned also suffers from heart problems, these are treated. The further course of the disease in most cases depends on the cause of the hyponatremia.
When should you go to the doctor?
If symptoms such as muscle spasms, seizures, and lethargy are noted, hyponatraemia may be the underlying cause. A doctor’s visit is indicated if the symptoms persist for more than a week or recur every few months. At the latest when other symptoms appear, medical advice is required. Nausea and vomiting, headaches and changes in behavior must be clarified immediately. If tremor attacks or epileptic seizures occur, friends and relatives or the person affected must call the emergency doctor themselves. In severe cases, first aid must be given until the doctor arrives.
Other warning signs that require clarification are tiredness, confusion and gait disorders. Frequent bone fractures also indicate hyponatremia and should be evaluated by a doctor. Individuals found to be sodium deficient are particularly prone to developing hyponatremia. If the symptoms mentioned appear after excessive consumption of water, gastric lavage or in the context of psychogenic polydipsia, medical advice is required. People who regularly take diuretics or ACE inhibitors should tell their doctor about any unusual symptoms.
Treatment & Therapy
The treatment of hyponatremia depends on the type and cause of the electrolyte imbalance. If hypovolemic hyponatremia is present, volume replacement with isotonic NaCl solution takes place. On the other hand, if it is the normovolemic form, there is a partial and slow administration of sodium. In the event of hypervolemia, the supply of water to the patient’s body is limited. In some cases, the administration of table salt can also be useful.
This is done either via the gastrointestinal tract or as an infusion. To avoid central pontine myelinolysis, it is important to balance sodium levels slowly and gently. This requires regular laboratory tests. Discontinuing medications, such as thiazide diuretics, is often sufficient for mild hyponatremia. In addition, it also helps treat heart failure or limit excess water intake, depending on the underlying cause.
In cases of hypervolemic hyponatraemia, a combination of saline and loop diuretics is sometimes helpful. Some patients require hemofiltration.
Prevention
Athletes can prevent hyponatremia by avoiding drinking too much water before a competition. It makes sense to drink 150 to 300 milliliters of water every 15 to 20 minutes during a competition, which corresponds to a small cup.
Aftercare
After treatment for hyponatremia, it is important for patients to find out about prophylaxis and aftercare options. The condition often occurs in combination with drinking too much water. Aftercare is therefore about consciously paying attention to the amount you drink.
This is the only way those affected can control their electrolyte balance. Those who suffer from the disease more frequently can minimize the risk by taking sodium supplements. Doctors prescribe these drugs and provide patients with precise dosage instructions. Those affected should also adhere to these so that they take the right amount.
These supplements are also available over the counter in pharmacies and drugstores. However, for individual follow-up care, patients should always speak to their doctor to avoid dosing errors. Depending on the cause of the disease, follow-up care can also extend to follow-up therapy for the underlying disease.
This often includes follow-up examinations in connection with kidney problems or cardiovascular complications. Short-term solutions tend to be used after an acute illness. Longer-term follow-up treatments are usually irrelevant. However, sufferers should not forget to monitor their sodium intake.
You can do that yourself
In many cases, hyponatremia can be avoided. If those affected are athletes, it is advisable for them to drink water in small quantities before competitions. The water supply should preferably take place every 20 minutes with 200 milliliters each time in order to create a balanced electrolyte balance. In most cases, this corresponds to an ordinary cup of water.
When treating hyponatremia, people can limit the disease by taking the sodium in supplement form. These can be prescribed by a doctor or purchased directly from a drugstore or pharmacy. However, the patient should always consult the doctor in order not to take in too much sodium.
If the disease has other causes, in most cases the underlying disease is treated first. Since those affected often suffer from kidney problems or heart problems due to hyponatremia, these organs should be examined regularly. This can avoid further complications. Furthermore, hyponatremia can be treated in acute conditions by limiting water intake. However, this should not be a long-term treatment.